Knee pain is one of the most common reasons runners stop training. The challenge is that "knee pain" can describe several different injuries, each with different triggers, treatment, and return-to-running timelines.
01Understanding knee pain in running
Not all running-related knee pain means "damage," and not all pain patterns need the same rehab plan. In many runners, pain shows up after a quick jump in load: more weekly mileage, extra hill sessions, increased speed work, a race block, or returning too fast after time off. In others, the issue is less about volume and more about specific stress—like repeated downhill running, sharp corners on a track, or strength deficits that shift load toward one tissue.
The goal of this guide is to help you build a better first hypothesis: where the pain is, how it behaves, and what activities make it better or worse. That first hypothesis helps you make smarter early decisions, such as reducing the right training variables, choosing better cross-training, and seeking assessment sooner when warning signs appear.
You do not need to self-diagnose perfectly to improve. You do need a structured approach. Think in this order: location, behavior under load, and 24-hour response. If your pain settles with modified load and steadily improves week to week, you're likely on the right track. If it persists, escalates, or includes red flag symptoms, get a formal clinical assessment.
02Quick symptom check
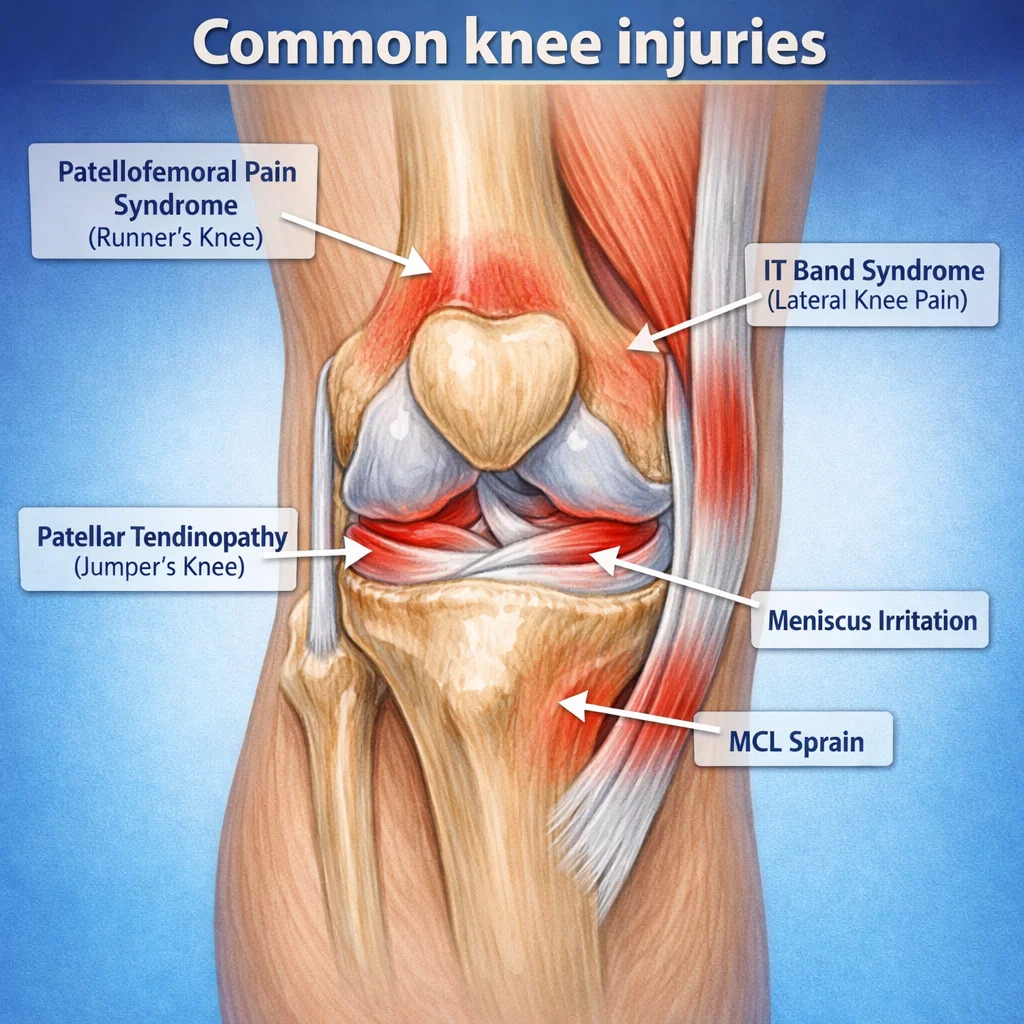
- Outside of knee pain, worse downhill: often points to IT band irritation.
- Pain around or behind kneecap: often patellofemoral pain syndrome.
- Pain at the tendon below kneecap: often patellar tendinopathy.
- Pain on inner knee after a twist: meniscus irritation or MCL sprain can be involved.
- Swelling or locking/catching: more likely joint involvement than simple overload.
These patterns are useful clues, not a diagnosis. Two runners can have similar pain locations but different underlying drivers (load, strength, mobility, or running mechanics). If symptoms are severe, recurrent, or not improving after 2-3 weeks of sensible load modification, get assessed by a sports physio or sports medicine clinician.
03Most common knee injuries in runners
Patellofemoral pain syndrome (runner's knee)
Usually felt as a dull ache around the kneecap. It often worsens with stairs, squats, downhill running, or after sitting with bent knees for long periods.
IT band syndrome (lateral knee pain)
Typically felt on the outside of the knee, often starting after a predictable distance into a run. Symptoms may settle quickly when you stop, then return as soon as you run again. For a full deep-dive on this condition, read our IT Band Syndrome guide.
Patellar tendinopathy (jumper's knee)
Usually a localized pain in the patellar tendon just below the kneecap. It is often load-sensitive, meaning symptoms rise with fast running, hills, and plyometrics.
Medial Meniscus Tear
Often linked to a twist or deep loaded knee bend. Pain is commonly felt along the inner joint line and can include clicking, catching, swelling, or a sense that full bend/straighten is blocked.
MCL Injury (Medial Collateral Ligament)
Usually pain on the inner knee after a sideways force or awkward step. The knee may feel tender to touch on the inside and unstable in early stages.
Pes Anserine Bursitis
Pain and tenderness are usually felt on the inner front part of the shin just below the knee joint. Symptoms often flare with uphill running, stairs, or when the area is pressed directly.
Baker's Cyst
Often presents as tightness, pressure, or a lump-like swelling behind the knee. It may feel worse with deep knee bend, longer runs, or after activity when the back of the knee feels full.
04Self-checks that can help narrow it down
- Location test: Use one finger to point to the most painful spot. Diffuse pain often means something different than a pinpoint tendon pain.
- Load test: Compare easy flat running vs hills, stairs, and squats. Different tissues react to different loads.
- Timing test: Note whether pain starts immediately, after a set distance, or several hours after running.
- 24-hour response: If pain and stiffness are clearly worse the next day, your current load is likely too high.
05Red flags: get assessed promptly
- Rapid swelling after injury.
- Knee giving way, locking, or inability to fully straighten.
- Night pain, fever, or unexplained weight loss.
- Pain after trauma where you cannot bear weight.
06What to do next
- Reduce load for 3-7 days by trimming the highest irritants first (speed, hills, long runs, or downhills).
- Keep pain-monitored movement (walking, light cycling, and easy strength) to maintain tissue tolerance.
- Restart running with shorter, flatter runs at easy effort and use small weekly increases.
- Track your 24-hour response after each run; if next-day pain spikes, reduce progression.
- If symptoms persist beyond 2-3 weeks, or worsen despite adjustments, seek a professional assessment.
Most running-related knee pain improves with smart load management and progressive strengthening. Early identification helps you choose the right rehab pathway sooner.
Sources and review
Last editorial source check: June 19, 2026. This injury guide is educational and has not yet been independently medically reviewed.
- Claims about runner knee pain patterns, hip and knee strengthening, education, and referral caution are informed by JOSPT's patellofemoral pain clinical practice guideline.
- Running-load advice is cross-checked against BJSM's youth running consensus statement and PubMed-indexed running-injury literature.
Last updated: June 19, 2026
Disclaimer: This article provides general information only and is not medical advice. Seek professional care for persistent or severe symptoms.
Learn how RunCalcs reviews health, injury, recovery, and nutrition content in our medical review policy.